
- Condition of the shoulder characterized by functional loss of passive and active shoulder motion
- The etiology is unclear
Epidemiology
- Affects females more than males
- More common in 40-60 year olds
Etiology/risk factors
- Primary adhesive capsulitis (AC) is idiopathic
- Post-traumatic – following proximal humerus fracture
- Post-surgical – following rotator cuff repair or axillary dissection
- Risk factors include several systemic diseases – e.g. diabetes mellitus, connective tissue disease, thyroid disorders, autoimmune disease
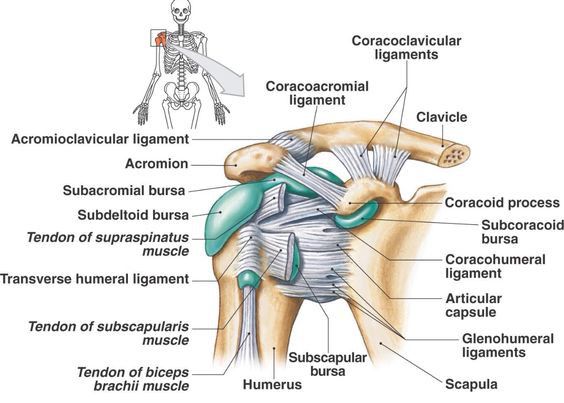
- The joint capsule is a fibrous sheath which encloses the structures of the shoulder joint
- The capsule is formed by the glenohumeral (GH) ligaments
- Glenohumeral ligaments – superior, middle and inferior
- Main source of stability for the shoulder, prevent it from dislocating anteriorly
- The is a triangular region between the anterior border of supraspinatus and superior border of subscapularis
- Contains the superior glenohumeral ligament and the coracohumeral ligament
Pathoanatomy
- Inflammation and fibroblastic proliferation of the joint capsule – leads to thickening, fibrosis and adherence of the capsule to itself and the humerus
- There is an abundance of fibroblasts and type III collagen
- Leads to a mechanical block to motion
- Reduction in synovial fluid which normally lubricates the joint
- Thickening and fibrosis of the rotator cuff interval – leads to contractions and fibrosis of the GH ligaments
Classification
Clinical stages
- Freezing/painful – gradual onset of diffuse pain
- Frozen/stiff – decreased range of motion affecting daily activities
- Thawing – gradual return of motion
Arthroscopic changes
- Stage 1 – patchy, fibrinous synovitis
- Stage 2 – capsular contractions and fibrinous adhesions
- Stage 3 – increasing contraction, synovitis resolving
- Stage 4 – severe contraction
Clinical features
- Insidious onset of generalised shoulder pain
- Variable severity of pain and loss of motion, depending on stage of presentation (see classification)
- Pain at rest and difficulty sleeping
Diagnosis
Physical exam
- Symmetric loss of active and passive range of motion
- External rotation deficit is most common
X-ray
- To rule out osteoarthritis/dislocation
Treatment
- Physiotherapy
- NSAIDs
- Heat/cryo-therapy
- Intra-articular steroid injections
Operative – to release adhesions
- Manipulation under anaesthesia (MUA) – to break up adhesions
- Higher rate of failure in diabetic patients
- Arthroscopic or open capsular release