
1. ANATOMY OF ANTERIOR ABDOMINAL WALL
Layers of the Anterior Abdominal Wall (from superficial to deep)
- Skin
- Subcutaneous tissue
- Fascia
- Camper’s fascia – fatty superficial layer
- Scarpa’s fascia – deep fibrous layer
- Muscles
- External oblique (EO)
- Internal oblique (IO)
- Rectus abdominis muscle
- Transverse abdominis (TA)
- Fascia transversalis
- Peritoneum
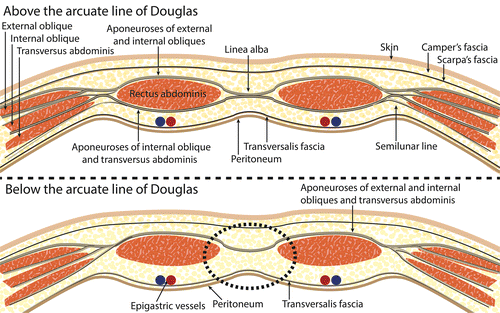
Rectus sheath
- All 3 muscle layers (EO, IO, TA) form an aponeurosis to surround the rectus abdominis – called the rectus sheath
- Arcuate line of Douglas – located at one third of the distance from the pubic crest to the umbilicus
- Demarcation where the IO and TA aponeuroses of the rectus sheath start to pass anteriorly to the RA, leaving only the TF to pass posteriorly (see pic)
Arterial supply of the anterior abdominal wall

2. HERNIAS
- Protrusion of peritoneum through an opening
- Due to structural weakness and increased intra-abdominal pressure
Etiology
- Straining, lifting of heavy weights
- Chronic cough – TB, asthma
- Chronic constipation
- Urinary causes – benign prostatic hyperplasia, prostate carcinoma, urethral stricture
- Obesity, pregnancy
- Smoking, ascites
Parts of a hernia
- Comprises of – covering, sac and contents
- Coverings – layers of the abdominal wall through which the sac passes
- Sac – diverticulum of peritoneum with mouth, neck, body, fundus
- Epigastric hernias lack a sac
- Contents (see below)
Classfication
Clinical classifcation
- Reducible – hernia can be pushed back
- Irreducible – cannot be pushed back
- Incarcerated – content of hernial sac are stuck inside it by adhesions
- Obstructed – bowel content cannot pass due to hernia, leads to distension, vomiting, constipation
- Strangulated – ischemia of tissue inside the hernia; patients becomes toxic and requires surgery urgently
Classficiation according to the contents
- Omentocele – omentum
- Enterocele – intestine
- Cystocele – urinary bladder
- Littre’s hernia – Meckel’s diverticulum
- Richter’s hernia – only the antimesenteric wall of the bowel herniates without compromising the entire lumen
- Maydl’s hernia – presence of two small bowel loops within a single hernial sac, more prone to strangulation and necrosis
- Sliding hernia – protrusion of a retroperitoneal organ through an abdominal wall defect
Classification based on site
- Inguinal hernia
- Femoral hernia
- Obturator hernia
- Diaphragmatic hernia
- Lumbar hernia
- Spigelian hernia
- Umbilical hernia
- Epigastric hernia
3. CONGENITAL DEFECTS OF THE ANTERIOR ABDOMINAL WALL
Omphalocele
- Defect is through the umbilicus
- Failure of the gut to return to the coelomic cavity during early fetal life due to malrotation
- The sac covering the contents is thin and consits of three layers
- Amniotic membrane, Wharton’s jelly and perionteal layer
Assoicated conditions
- Congenital abnormalities
- Congenital heart defects
- Neural tube defects
- Exstrophy of the bladder
- Beckwith-Wiedemann syndrome – an overgrowth syndrome characterised by several findings
- Macrosomia, macroglossia, omphalocele, visceromegaly, embryonal tumour, renal abnormalities
- Chromosomal anomalies
- Trisomies 13, 15, 18, 21
Pathophysiology/clinical features
- Omphalocele minor
- The sac is small and the umbilic cord is attached to the summit
- Can be treated by twsiting the sac and reducing the contents to the peritoneal cavity through the umbilical defect
- Omphalocele major
- Presents with a large defect (5cm), with contents lying completely outside
- Contents – small intestine, large intestine, liver
- The sac can rupture during devliery, leading to infection and high mortalitity
- It is not possible to reduce the contents to the peritoneal cavity as the abdominal cavity is not developed properly – if contents are forced into the cavity it can lead to intestinal obstruction or respiratory distress
- A sterile bag is wrapped over the contents and contents are gradually twisted over 2-3 weeks to stimulate the peritoneal cavity to increase in capacity
- Antibiotics, fluids and nutritional support is required throughout this process
Gastroschisis
- Defect is lateral to the umbilicus
- Common in preterm babies
- Associated with defect in the involution of the 2nd umbilican vein
- Risk factors – mothers <20 years, smoking, alcohol, intake of aspirin and ibuprofen during first trimester
Pathophysiology/clincial features
- Incomplete development of the anterior abdoinal wall results in a defect which allows abdominal organs (normaly intestines) to produce through the abdominal wall
- Intestines herniate through the rectus abdominis muscle, lying to the right of the umbilicus
- There is no peritoneal sac so the irritating effect of amniotic fluid causes chemical peritonitis with formation of a thick, edematous membrane
- After birth, infants are more prone to fluid loss, hypothermia, sepsis
- They are also more susceptible to developing necrotising enterocolitis
Treatment
- General – fluids, antibiotics, caloric supplementation
- Surgical
- Initially the bowel is placed in a sterile bag
Later, the intesintes are pushed into the abdomen through the defect and the defect is closed