
Congenital hip joint luxation (DDH)
- Disorder in which the acetabular and femoral head are misaligned resulting in unstable hip – usually present at birth but sometimes can present later as the hip develops
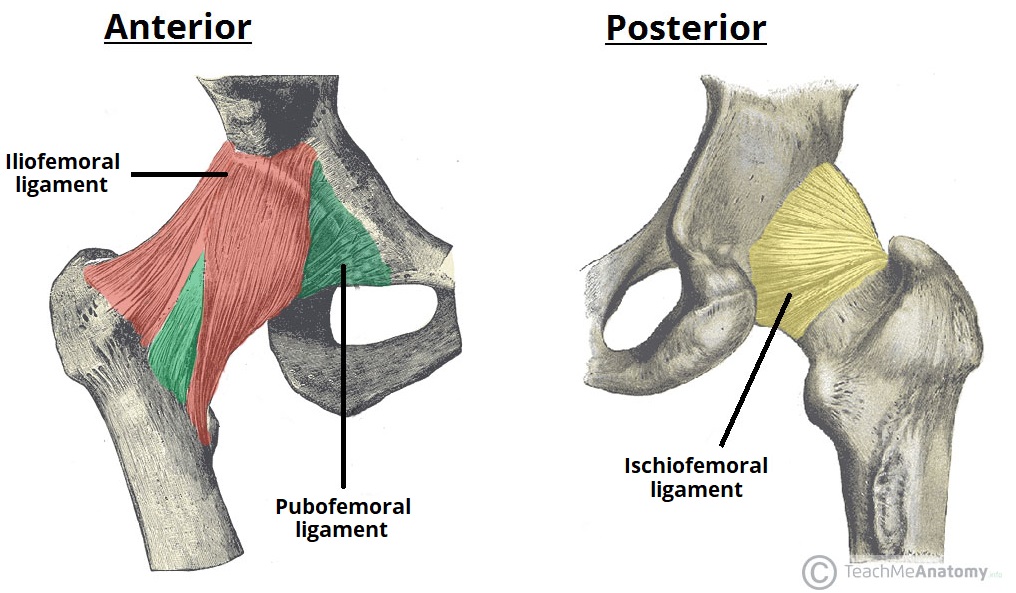
- The hip joint has – the ileofemoral, pubofemoral and ischiofemoral
- the main function is to articulate bones together and stabilise the hip joint when moving
Epidemiology
- Most common congenital abnormality of skeletal development
- More common in females
- Most common in the left hip
Etiology/Risk factors
- First born
- Breech
- Family history
- Oligohydraminos
- Macrosomia
Pathophysiology
- Initial instability is due to the risk factors → leads to dysplasia → leads to subluxation and eventually dislocation
- Chronic dislocation leads to
- Further difficulty in reduction – thickening of thickening of ligamentum teres; hypertrophy of the transverse acetabular ligament
- Anatomic changes – flattening of the femoral head, femoral anteversion, decreased concavity of acetabular roof
Spectrum of disease
- Dysplasia – shallow or underdeveloped acetabulum
- Subluxation – displaced joint, with some contact between articulating surfaces
- Dislocation – completely displaced joint, with no contact between articulating surfaces
- Teratologic hip – dislocated in utero, presents with
- Adolescent dysplasia – stable and reduced but dysplastic
Classification
- Subluxable – Barlow-suggestive
- Dislocatable – Barlow-positive
- Dislocated – Ortolani-positive when reducible (early); Ortolani-negative when irreducible (late)
Clinical features
- Gluteal fold asymmetry
- Abduction range asymmetry
Physical exam
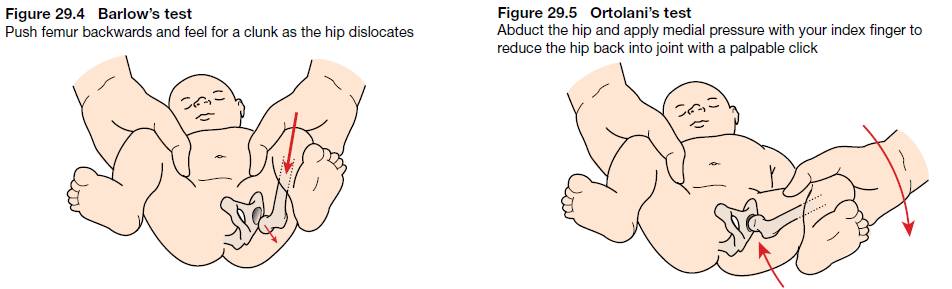
- Under 3 months
- – adduct hip and apply pressure to push back and dislocate the femur
- Felt by a ‘click’ when femur exits the joint as it dislocates
- – abduct the hip and elevate the femur to reduce it back into the hip joint
- Felt by a ‘click’ when femur enters the joint as it reduces
- – adduct hip and apply pressure to push back and dislocate the femur
- 3 months – 1 year
- Limitation in hip abduction – most sensitive test
- Discrepancy in leg length
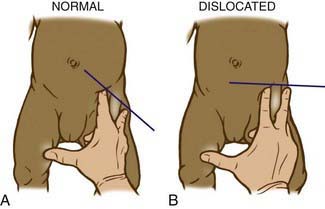
- – middle finger placed over greater trochanter, index finger placed over ASIS
- Normal – should point towards the umbilicus
- Dislocated – points halfway between umbilicus and pubis
- Over 1 year
- Pelvic obliquity
- Lumbar lordosis
- Trendelenburg gait
- Toe-walking
Imaging
– after 4-6 months when femoral head begins to ossify
- Dislocation
- 2 lines are drawn on the X-ray
- Hilgenreiner’s line – across the triradiate cartilages of the acetabulae
- Perkin’s line – perpendicular to H line, passes through lateral edge of the acetabular roof
- Normal – femoral head should lie in the inferomedial quadrant of these two lines
- 2 lines are drawn on the X-ray
- Dysplasia
- Acetabular Index – angle formed by H line and a line from a point on the lateral triradiate cartilage to a point on the lateral margin of acebulum
- Normal – should be <25o
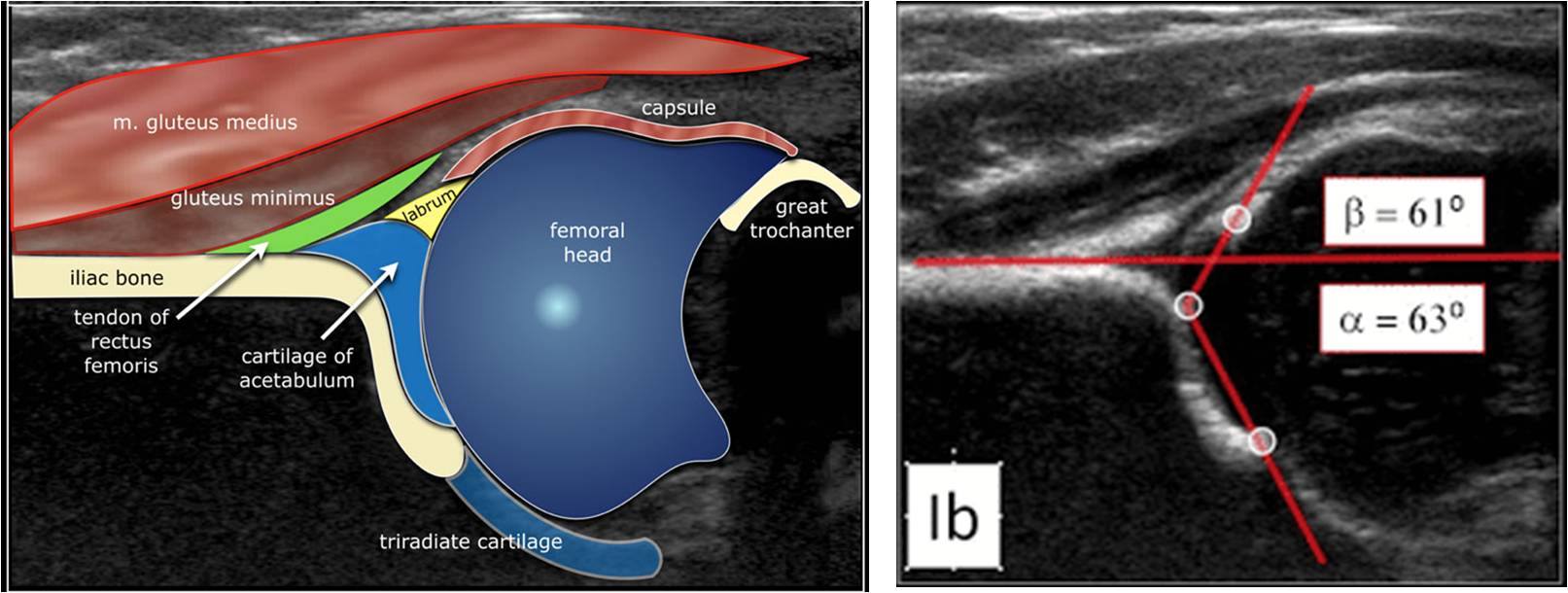
- Alpha angle – angle between the bony roof of the acetabulum and the ilium
- Should be >60o. Less than this indicates a shallow acetabulum
- Beta angle – angle between the labrum and the ilium
- Should be <55o
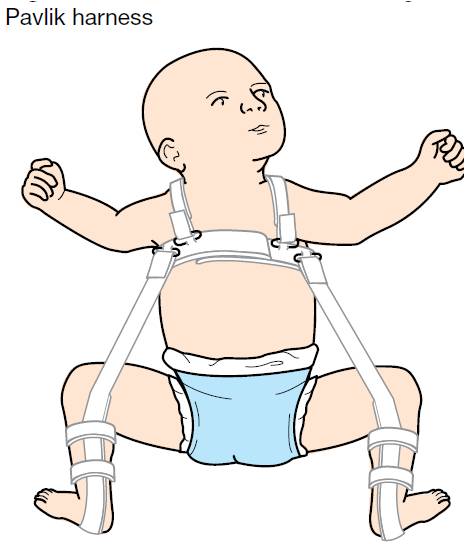
Treatment
- Under 6 months – : keeps the hip flexed and abducted; should be worn for 23 hours per day
- 6 – 18 months – closed reduction and spica casting
- Over 18 months – open reduction with femoral/pelvic osteotomy, followed by casting
Complications
- Avascular necrosis of the femoral head
- Femoral nerve palsy
- Osteoarthritis
- Asymmetric gait
- Decreased range of motion in hip joint