
DI may be due to lack of hormone ( Central ) or inadequate response to hormone ( Nephrogenic )
Physiology
– Normal concentrations cause reduction of diuresis in kidney tubules via aquaporin 2.
 – High concentration causes vasoconstriction in vascular tissue
– High concentration causes vasoconstriction in vascular tissue
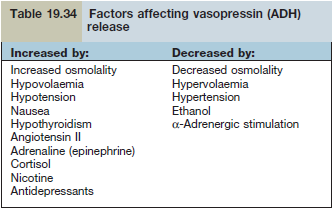
– ADH (anti- diuretic hormone) is supressed below 280mOsm/kg
– Max ADH action is achieved at 295 mOsm/kg
– Thirst is achieved at 295 mOsm/kg
Etiology- Central – idiopathic, head trauma, vascular disorders,
- Nephrogenic – idiopathic, hypercalcemia, hypokalaemia, chronic kidney disease, pregnancy
- Congenital – Wolfram syndrome (WFS1 mut) – DI, DM, optic atrophy, deafness
Clinical features
- Polyuria, nocturia, polydipsia, dehydration, impaired consciousness
- DI may be masked by cortisol deficiency. Give hydrocortisone to see if DI apparent (symptoms still present)
Diagnosis
- Fluid deprivation test
-
- Healthy patients
- Normal plasma osmolality and increased urine (600 mOsm/kg)
- DI
- High plasma Osm and normal/low urine Osm.
- Corrected with Desmopressin (cranial)
- If not corrected (nephrogenic)
- Healthy patients
Treatment
- Desmopressin – intranasal [20-40mcg], oral [100-200mcg], I.M
- Doesn’t cause vasoconstriction.
- Thiazides
- Sensitise s renal collecting ducts. Good for nephrogenic type.