
- Herniation of abdominal content through diaphragm into the chest
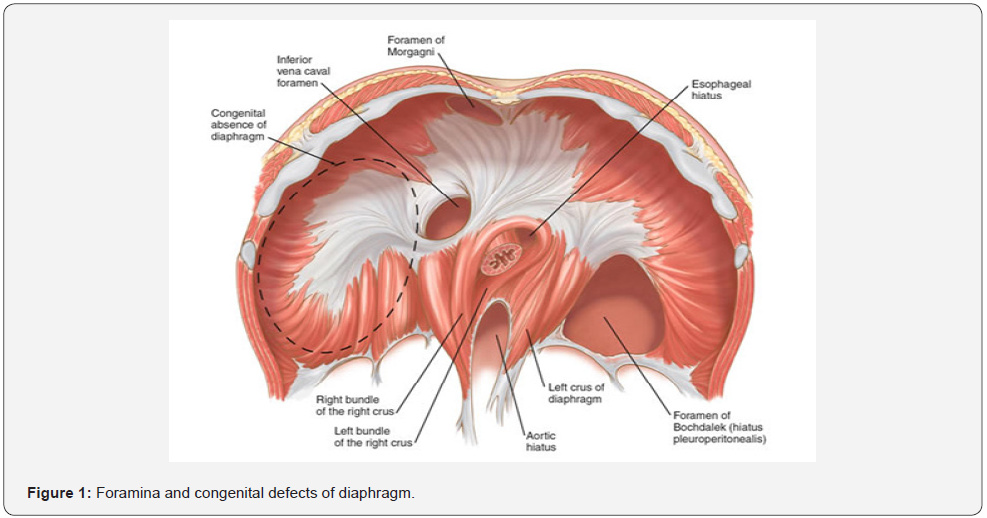
Anatomy – foramina of the diaphragm
Classification of diaphragmatic hernias
Congenital
- Bochdalek hernia – most common congenital type
- Morgagni hernia
- Diaphragm eventration
Acquired
- Traumatic
- Hiatus hernia – most common type of diaphragmatic hernia
- Iatrogenic
Bochdalek Hernia
- Defect is more common on the left hand side, posteriorly
Pathogenesis
- It is a developmental defect which occurs due to failure of fusion of pleuroperitoneal canal leaving a direct communication between pleura and peritoneum – allows herniation of abdominal contents into the chest cavity
- Abdominal contents can be – colon, small intestine, stomach
- Leads to decreased total lung mass and pulmonary hypoplasia
- 80% cases do not have hernia sac
Clinical features
- Symptoms usually present in the newborn period
- Respiratory issues, cyanosis, tachycardia
- Scaphoid abdomen
- Bowel sounds in the left hand side of chest
- Mediastinal shift to the right hand side
- Intestinal obstruction
Investigations
- CXR, barium enema/meal, ABG
Treatment
- Respiratory support
- Laparotomy and dissection of the sac with closure of the defect in diaphragm
Hernia through Foramen of Morgagni
- Defect is more common on the right hand side, anteriorly
- Contents – omental fat or colon
- It usually asymptomatic, but can present with respiratory problems and recurrent chest infections
- Can be treated with laparoscopic repair if asymptomatic
Eventration
- Weakening of diaphragm due to atrophy and loss of muscle with fibrous tissue formation
- Diaphragm is attenuated and inactive
- Classification of eventration
- Congenital – marked decrease in the muscle fibres in the diaphragm
- Acquired – (a) phrenic nerve palsy due to trauma (b) viral i.e. polio, HZV, influenza (c) neoplasia (d) autoimmune neuropathy (d) iatrogenic
- Often present in infancy and childhood
- The thin diaphragm is raised higher and immobile – it is not actually a true herniation but features mimic hernia
Clinical features
- Can be asymptomatic
- Wheezing, recurrent lower respiratory tract infections, extreme respiratory distress, V/Q mismatch
Investigations
- CXR/CT/MRI
- Pulmonary function tests
Treatment
- Diaphragmatic plication
Traumatic diaphragmatic hernia
- Can occur either on the left and right hand side
- Etiology – road traffic accident, crush injuries, penetrating injuries or blunt injuries
- Most commonly herniated organs – stomach and colon
- Patient is pale, has respiratory distress, guarding and rigidity over the abdomen
Oesophageal hiatus hernia
- Hiatus – hole through diaphragm where oesophagus passes through into stomach
Etiology
- Idiopathic
- Increasing age
- Increase pressure in the abdomen from – pregnancy, obesity, coughing, straining, ascites
- Sliding hernia – type I
- Upward dislocation of the cardia through the oesophageal hiatus
- Gastro-oesophageal junction (GOJ) protrudes into chest
- Most common type of hiatal hernia
- Rolling hernia/paraoesophagel hernia (PEH) – Type II
- Upward dislocation of the gastric fundus alongside a normally positioned cardia
- GOJ is in its normal location, but the fundus passes/bulges into chest beside the oesophagus
- Mixed type – has both a sliding and rolling component
Clinical features
- Most cases are asymptomatic
- Symptoms of GORD – heartburn, epigastric pain
- Vomiting, weight loss
- Severe cases – bleeding, dysphagia, chest pain
Investigations
- Oesophagogastroduodenoscopy – gold standard
- Barium swallow
- CT, MRI
Treatment
- Conservative – omeprazole (PPI), weight loss, diet modification, smoking cessation
- Surgical – indicated when there is increased risk of strangulation/volvulus
- Cruroplasty – hernia is reduced from the thorax into the abdomen; may require mesh
- Fundoplication – fundus is wrapped around and sutured to the lower oesophagus, to strengthen the lower oesophageal sphincter
Internal hernias
- Protrusions of the viscera through the peritoneum or mesentery but remaining within the abdominal cavity
- Acute small bowel obstruction is the most common presentation
Etiology – pathologic defects of the mesentery and visceral peritoneum
- Congenital maldevelopment of mesenteries
- Iatrogenic – surgery
Types
- Paraduodenal hernias
- Lesser sac (foramen of Winslow) hernias
- Pericaecal hernia
- Sigmoid mesocolon hernia
- Falciform ligament hernia
Investigations
- CT – gold standard; shows encapsulation of distended bowel loops within an abnormal location
- Barium studies
Treatment
- Surgery to release the constricting agent by division