
1. ANATOMY OF INGUINAL CANAL
- Deep inguinal ring – located at the halfway point of inguinal ligament
- Provides an entrance for abdominal contents to exit
- Contents in males – spermatic cord and ilioinguinal nerve
- Contents in females – round ligament of the uterus and ilioinguinal nerve
- Provides an entrance for abdominal contents to exit
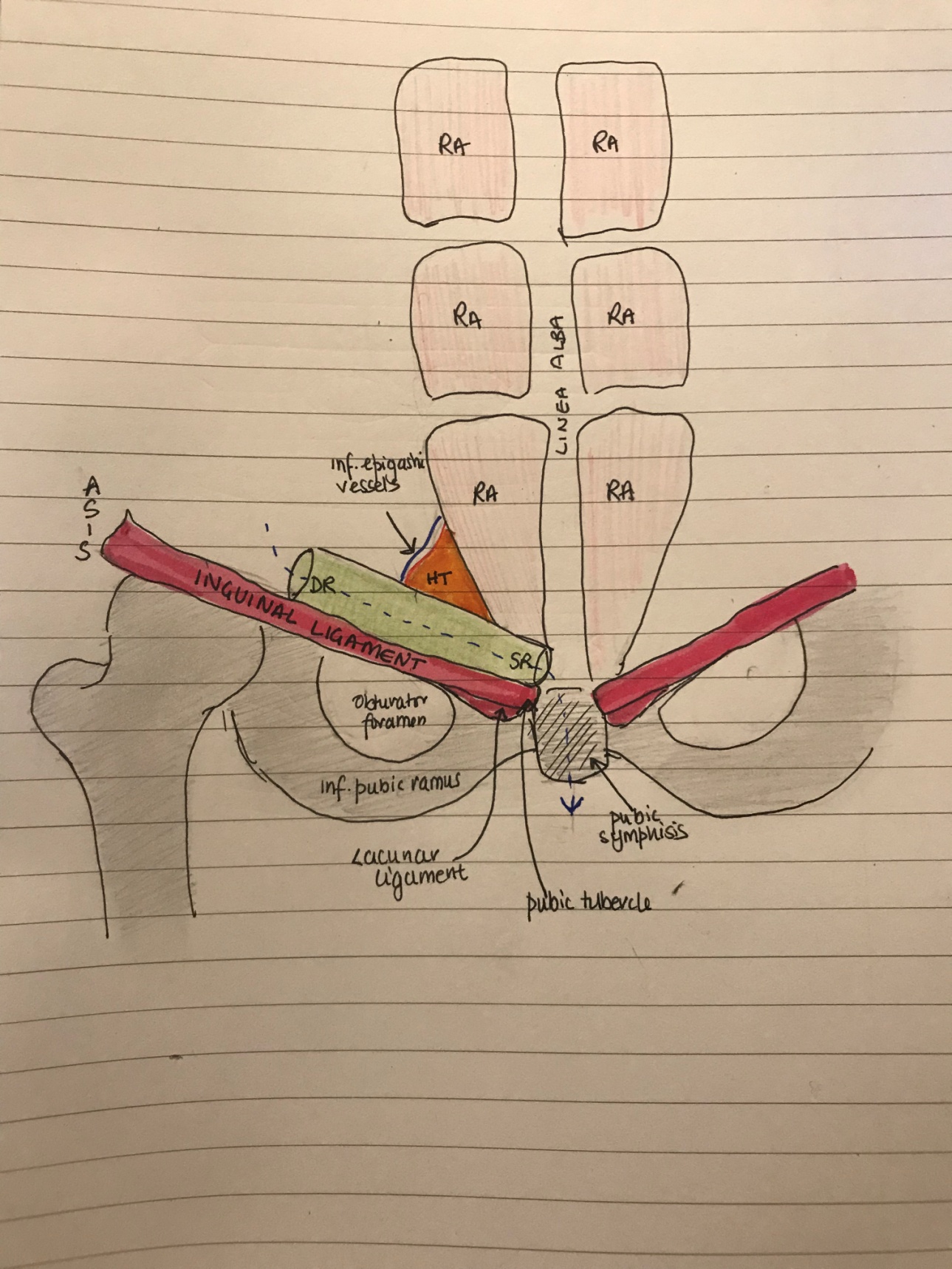
- Hesselbach’s triangle
- Medially – rectus abdominis
- Laterally – inferior epigastric vessels
- Inferiorly – ilioinguinal ligament
- Walls of inguinal canal – MALT
- M – superior (roof)
- 2 MUSCLES – Internal oblique and transverse abdominis
- A – anterior
- 2 APONEUROSES – internal oblique and external oblique
- L – inferior (floor)
- 2 LIGAMENTS – Inguinal ligament + lacunar ligament
- T – posterior
- 2 Ts – Transverse fascia + conjoint tendon medially
- M – superior (roof)
2. INGUINAL HERNIAS
Types of inguinal hernias
- Indirect – goes through deep inguinal ring, lateral to the inferior epigastric artery (IEA)
- Can descend into scrotum
- Most common in children
- Direct – occurs through posterior wall of inguinal canal through Hesselbach’s triangle, sac is medial to the IEA
- Cannot descend into scrotum
- Common in old age
- Incomplete
- Bubonocele – sac is confined to inguinal canal
- Funicular – sac crosses the superficial ring but doesn’t reach the bottom of the scrotum
- Complete – sac descends to bottom of the scrotum
According to content
- Eneterocele, omentocele, cystocele
Clinical types
- Reducible, irreducible, obstructed, strangulated
Rare type of inguinal hernias
- Sliding hernia – protrusion of a retroperitoneal organ through an abdominal wall defect
- Richter’s hernia – only the antimesenteric wall of the bowel herniates without compromising the entire lumen
- Littre’s hernia – hernia containing Meckel’s Diverticulum
- Maydl’s hernia – presence of two small bowel loops within a single hernial sac, more prone to strangulation and necrosis ()
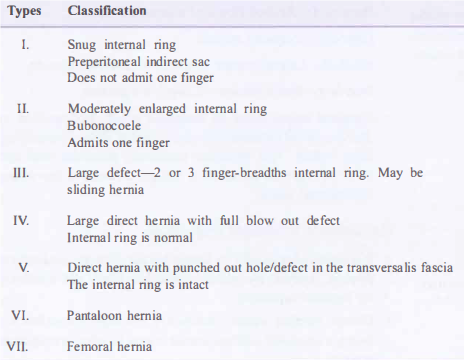
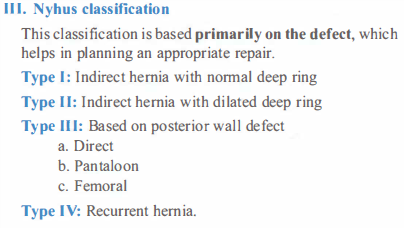
Classification of hernias
Gilbert’s Classification NYHUS Classification
Clinical features
- Most common in males
- Dragging pain and swelling in groin – better seen on coughing and standing
- Usually reducible
- Deep inguinal ring (DIR) occlusion test
- In lying down position, DIR is occluded with the thumb and patient is asked to cough
- If swelling appears medial to thumb – DIRECT HERNIA
- If swelling appears on releasing the thumb – INDIRECT HERNIA
Investigations
- Inspection – lump size, shape, position, scrotal extension, observe cough impulse
- Palpation – inguinal lump, feel scrotum
- Per rectal exam
- Reducibility
- Always feel the other side
Complications
- Recurrence
- Groin pain
- Haematoma
- Infection
- Testicular atrophy
- Contraction
- Seroma
Treatment
Open repairs
- Herniotomy (excision of hernial sac) and herniorrhapy/hernioplasty (strengthening of the posterior wall of the inguinal canal by repair or mesh)
- Bassini repair – approximation of the inguinal ligament to the conjoined tendon with sutures
- Shouldice – 4-layered repair of floor of inguinal canal with running sutures
- Lichtenstein repair – hernia gap closed using a synthetic mesh, which is sutured to the inguinal ligament
Laparoscopic repairs
- TAPP – transabdominal preperitoneal repair
- TEP – total extraperitoneal repair