Epidemiology/etiology
- MC malignant tumour worldwide
- Cigarette smoking accounts for >90% of cases
- Environmental – radon, asbestos, ionizing radiation
- Host factors – pulmonary fibrosis, HIV, genetics
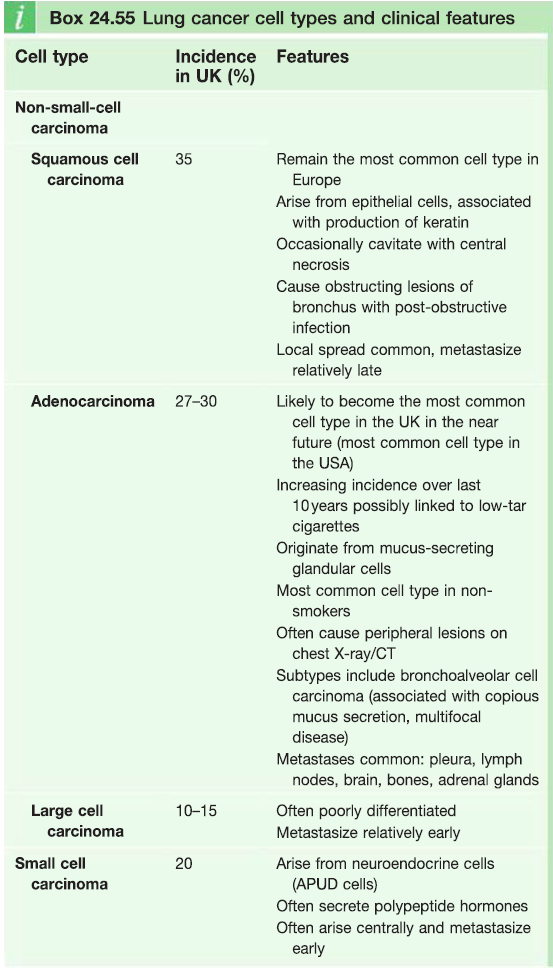
Classification – see box
- SCC (small cell cancer) – metastasise early
- NSCC (non-small cell cancer) – tend to be diagnosed in a localised form
Clinical features
Local effects
- Cough – for >3 weeks
- Breathlessness – due to airway occlusion
- Haemoptysis
- Chest pain – when tumour invades pleura
- Wheeze
- Hoarseness – compression of rec. laryngeal n
- Nerve compression
- Pancoast tumour in lung apex invades the brachial plexus – causes C8/T1 palsy, muscle wasting and hand weakness
- Recurrent infections
Metastatic spread
- Spreads to mediastinal, cervical, axillary lymph nodes
- Liver – anorexia, WL, nausea, RUQ pain
- Adrenal glands
- Bone – pathological fractures
- Brain – space occupying lesions with Mass effect ; symptoms – ↑ICP; headache
- Malignant pleural effusion
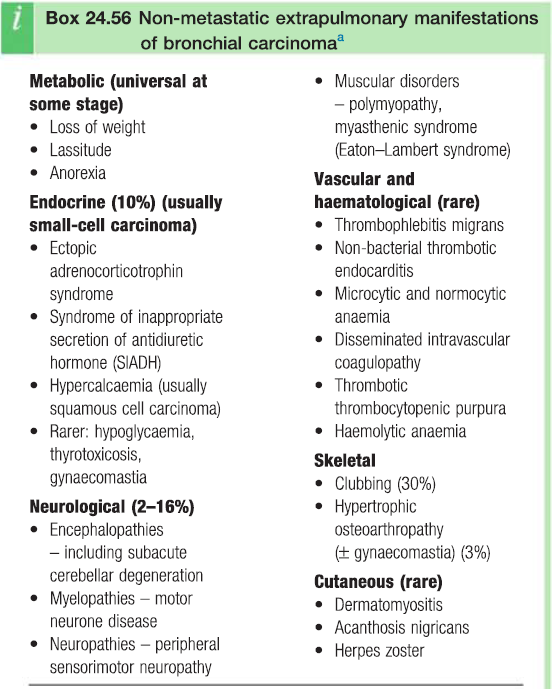
Non-metastatic extrapulmonary manifestations
- Metabolic – WL, anorexia
- Endocrine (SCC) – SIADH , gynaecomastia
- Neurological – MND , peripheral neuropathy
- Vascular – anaemia, DIC
- Skeletal – clubbing
Diagnosis
Aim
- Stage extent of disease
- Classify the tumour – SCC vs NSCC
- Assess fitness to undergo treatment
Investigations
- CT – shows extent of disease
- Include imaging of liver and adrenals
- PET – to show mediastinal LN involvement and distant mets
- Bronchoscopy – obtain biopsy
- If carcinoma involves the first 2cm of either main bronchus then the tumour is inoperable
- Percutaneous aspiration and biopsy
- Endobronchial ultrasound
- Others – FBC, LFTs
Staging
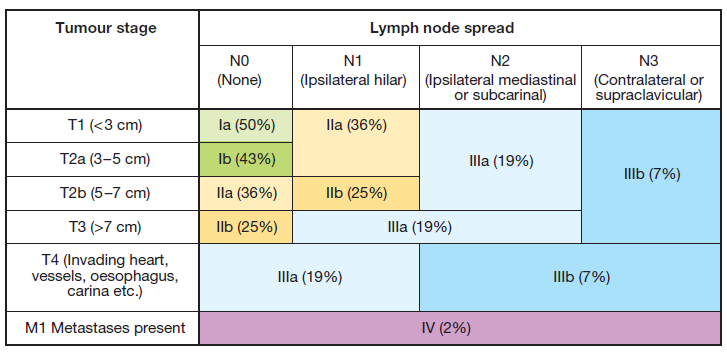
Notes
- TX – tumour cannot be assessed
- T0 – no evidence of tumour
- Tis – carcinoma in situ
- NX – regional LNs cannot be assessed
Complications