Epidemiology
- Rule of 2
- Occurs in 2% of the population
- 2 inches in length
- 2 feet from ileocaecal valve
- 2% of cases become symptomatic
- 2 types of ectopic tissue are present – mostly gastric and pancreatic
- More common in females
- May be associated with oesophageal atresia, exomphalos and anorectal malformations
Etiology
- Congenital diverticulum arising from the terminal ileum
- Due to unobliterated proximal portion of the vitello intestinal duct
- Vitello intestinal duct – connects midgut with the yolk sac during fetal development
- Normally this duct obliterates during the 9th gestational week
- Failure to obliterate can result in several types of vitelline fistula
- Meckel’s diverticulum (MD) is a viteline fistula which arises when the proximal portion (intestinal end) of the duct fails to obliterate
- Can be attached to the umbilicus by a fibrous cord
Pathophysiology
- MD is a true diverticulum – contains all layers of the bowel
- i.e. mucosa, muscularis propria and serosa
- The mucosa contains heterotrophic epithelium
- Most commonly gastric, colonic and pancreatic tissue
- It lies on the antimesenteric border of the ileum
- Has its own blood supply – via the vitelline artery (arises from an ileal branch of the superior mesenteric artery)
Clinical Presentation
- Can be asymptomatic – silent MD
- Painless rectal bleeding
- Intestinal obstruction due to
- Adhesions/band
- Volvulus
- Intussusception
- Littre’s hernia – a hernia containing a Meckel’s diverticulum
- Diverticulitis – mimics acute appendicitis
- Severe epigastric pain
Complications
- Peptic ulceration – form heterotrophic gastric epithelium
- Severe haemorrhage
- Perforation
- Neoplasm – carcinoid or GIST tumour
Diagnosis
- Tc99m radioisotope scan – identifies heterotropic gastric mucosa
- XR abdomen – to see complications like obstruction and perforation
- Small bowel enema under fluoroscopy
- CT angiography – to show patent vitelline artery
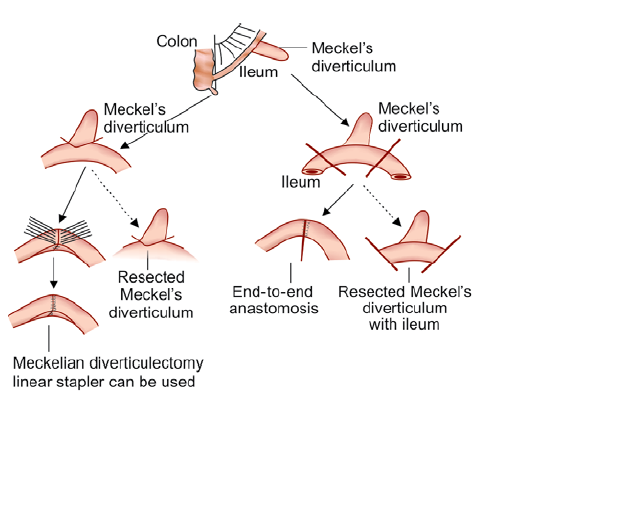
Treatment (see pic)
- Asymptomatic cases not require treatment
- Meckel’s diverticulectomy – in MD without complications
- Resection of MD and adjacent ileum with end-to-end anastomosis – in MD with complications (e.g. bleeding, strangulation, bowel obstruction)