
- Injury to the brachial plexus during birth
Epidemiology
- Less common in areas with good obstetric care
- In 1/1000 live births
Etiology
- Macrosomia
- Multiparous pregnancy
- Difficult presentation
- Forceps delivery
- Prolonged labour
- Associated conditions – glenohumeral dysplasia, torticollis, clavicle fracture
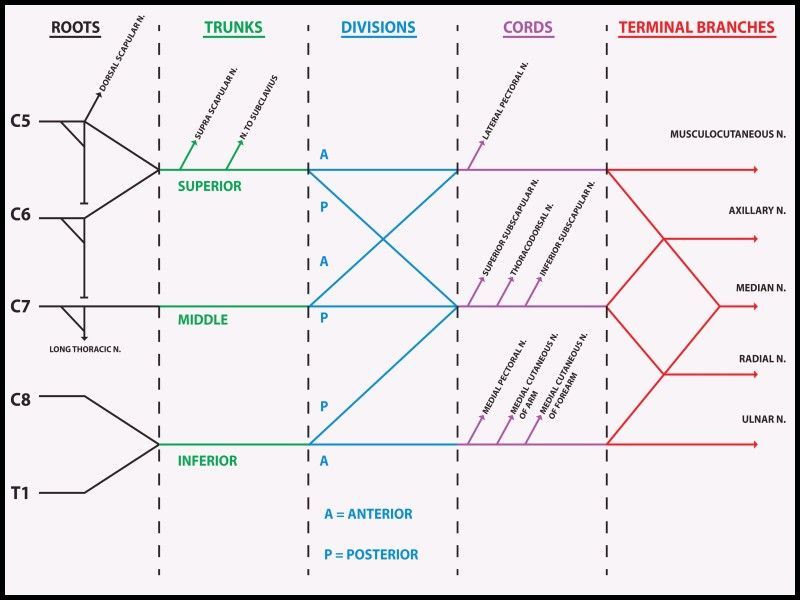
Anatomy
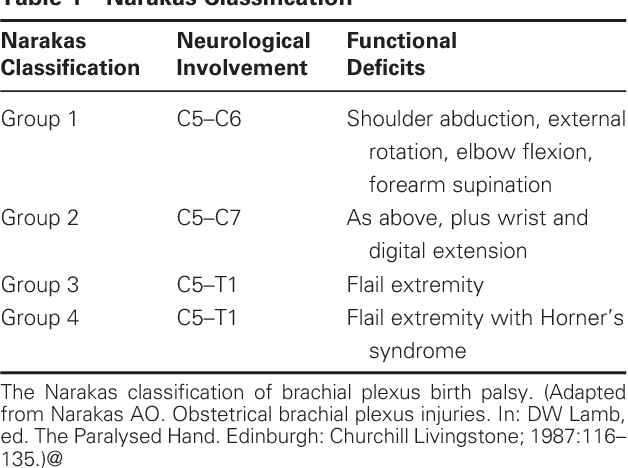
Classification – Narakas Classification
Types
Erb’s Palsy (most common)
- Affects C5, 6
- Mechanism
- Traction on plexus is caused by lateral flexion of the head towards the contralateral shoulder with depression of the ipsilateral shoulder
- Occurs during difficult delivery in infants
- Clinical features
- Adducted, internally rotated shoulder; pronated forearm, extended elbow
- C5 deficiency
- Axillary n. deficiency – deltoid and teres minor weakness
- Suprascapular n. deficiency – supraspinatus and infraspinatus weakness
- Musculocutaneous n. deficiency – biceps and brachialis weakness
- C6 deficiency
- Radial n. deficiency – brachioradialis and supinator weakness
- Best prognosis
Klumpke’s Palsy (rare)
- Affects C8, T1
- Mechanism
- Occurs in infant born with arm presentation, results in traction/abduction from trunk
- Clinical features
- Deficit of all of the intrinsic muscles in the hand – normally flex MCP joints and extend DIP and PIP joints
- – due to loss of opposing action of intrinsics
- Hyperextension of MCP
- Flexion of DIP and PIP
- Poor prognosis for spontaneous recovery
- Associated with Horner’s syndrome
Total Plexus Palsy
- Affects C5-T1
- Mechanism – due to stretch, rupture and avulsion injury
- Clinical features – flaccid arm; motor and sensory deficits
- Worst prognosis
Diagnosis
- XR – to evaluate clavicle/humerus fracture (may be unclear due to incomplete ossification in infants)
- CT/MRI
- USS – to assess joint subluxation or dislocation
Treatment
General
- Non-operative – daily passive exercises
- Operative
- Microsurgical nerve grafting
- Nerve transfer – fascicles from one nerve transferred into another nerve
Shoulder dislocation and contractures
- Hoffer procedure – latissimus dorsi (LD) and teres major (TM) transfer
- Transfer of LD and TM tendons to the rotator cuff – improves external rotation and adduction of shoulder
- Pectoralis major lengthening – to lesson internal rotation forces
- Arthrodesis – artificial induction of joint ossification between two bones by surgery
Elbow flexion contracture
- Non-op – serial elbow extension splinting/casting
- Op – anterior capsular release
Forearm, wrist, hand
- Tendon transfer