- Pleural effusions – accumulation of serous fluid within the pleural cavity
- Detected on X-ray when >300ml
- Detected clinically when >500ml
Pathophysiology
Transudate
- ↑capillary hydrostatic pressure
- ↓capillary oncotic pressure
Exudates
- ↑capillary permeability – e.g. due to inflammation
Transudates
- Can be bilateral – often larger on the right side
- Protein content <30g/L
- LDH <200IU/L
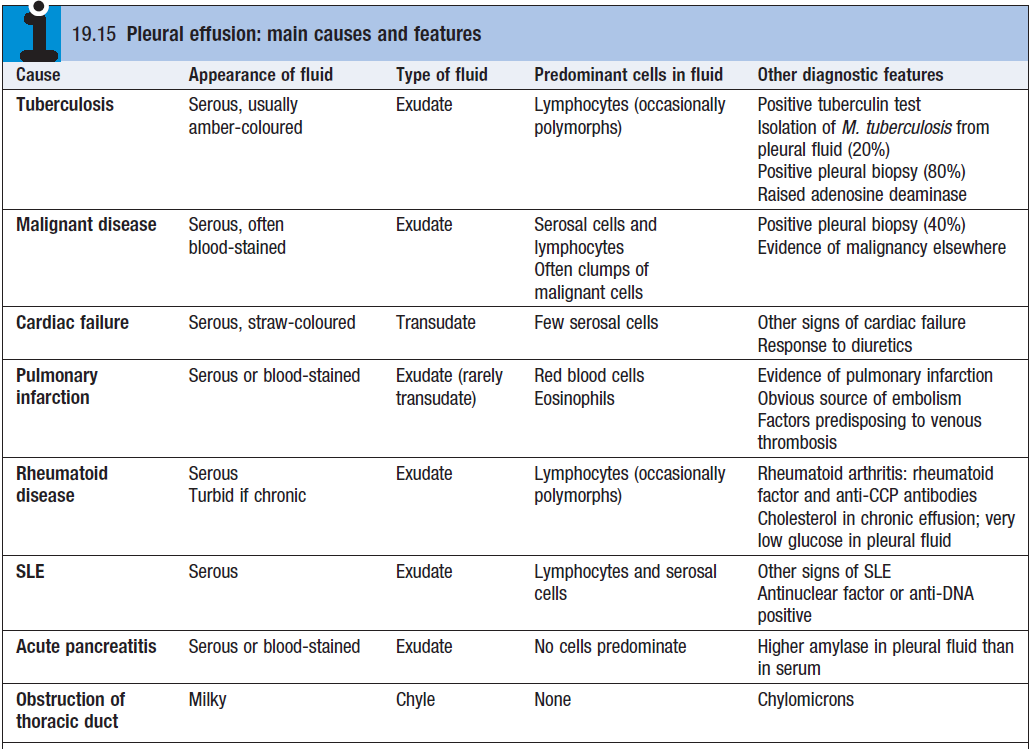
- Causes
- Heart failure
- Hypoproteinaemia (e.g. nephrotic syndrome)
- Constrictive pericarditis
- Hypothyroidism
- Ovarian tumours producing right-sided pleural effusion – Meigs syndrome
Exudates
- Protein >30g/L
- LDH >200IU/L
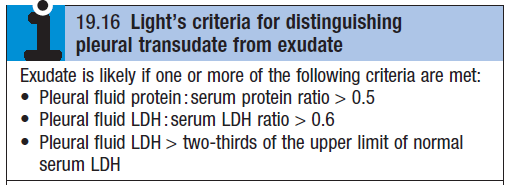
- Light’s criteria for diagnosis of an exudative effusion – see box
- Causes
- Bacterial pneumonia
- Bronchial carcinoma
- Tuberculosis
- Acute pancreatitis
Clinical features (if effusion is >500ml)
- Pain on inspiration
- Coughing
- Pleural rub
- Reduced chest wall expansion
- Reduced/absent breath sounds
Diagnosis
- CXR – curved shadow at lung base; blunting of costophrenic angle
- USS – more accurate than CXR
- Transudate – clear hypoechoic space
- Exudates – presence of moving floating densities
- Pleura aspiration – information on colour and texture of fluid
- Biopsy – pathological and microbiological analysis
Treatment
- Aspiration to relieve dyspnoea – fluid should be removed slowly as fast removal can cause pulmonary oedema
- Treat underlying cause