
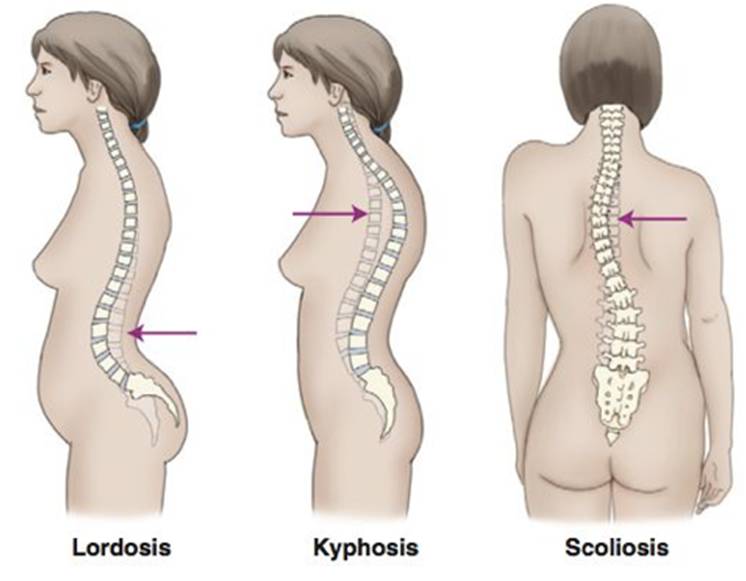
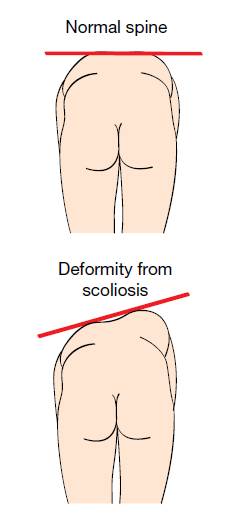
- Abnormal sideways curvature of the spine in an S or C shape resulting in uneven shoulders and hips
- Deformity of spine in 3 places – rotation, lateral bending,
Epidemiology
- Age of onset is usually 10-15 years
- More common in females
Etiology
- Combination of genetic and environmental factors
- 65% of cases are idiopathic, 15% are congenital, 10% are secondary to other conditions
Pathology
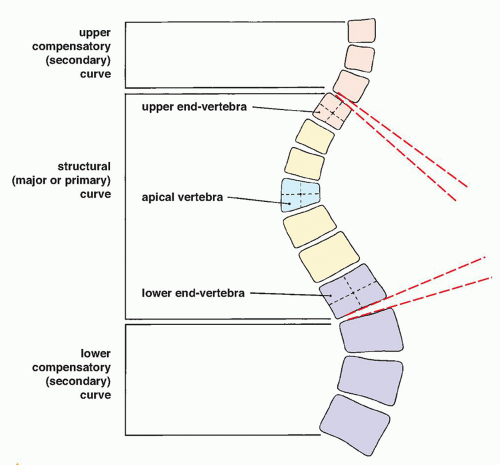
- The main pathology is the of the spine – called the primary curve
- There may be compensatory curvature above or below the primary curve – called the secondary curves
- Lateral curvature is due to rotation of the vertebrae
- When thoracic spine is affected, rotation leads to prominence of the rib cage on the convex side, giving the appearance of a ‘rib hump’
- Lumbar spine can also be affected
- Risk factors for curve progression
- Female sex
- Young age
- Premenarche
- Skeletal immaturity – assessed by Risser classification
- Cobb’s angle >50o
- Progression >5o over two consecutive X-rays
Classification
- Idiopathic scoliosis – most common. Associated with CHD7 and MATN1 genes
- Infantile – below 3 years
- Juvenile – 3-10 years
- Adolescent – over 10 years
- Congenital scoliosis
- Due to failure of normal vertebral development during 4-6th gestational week
- Neurogenic scoliosis
- Secondary to neuromuscular conditions – muscular dystrophy, poliomyelitis, celebral palsy
- Syndromic
- Associated with other syndromes – , fragile X, Prader-Willi etc
Clinical features
- Idiopathic scoliosis most commonly shows visible deformity but no pain
- Pain in back, shoulders, neck and ribs
- Respiratory problems
- Rib prominence/hump – in thoracic scoliosis
- Uneven leg length
- Café-au-lait spots – in neurofibromatosis
- Limited mobility
- Slow reflexes
Diagnosis
Physical exam
- – ask patient to bend forward at the waist and examiner looks at the level of the scapulae from behind the patient
X-ray
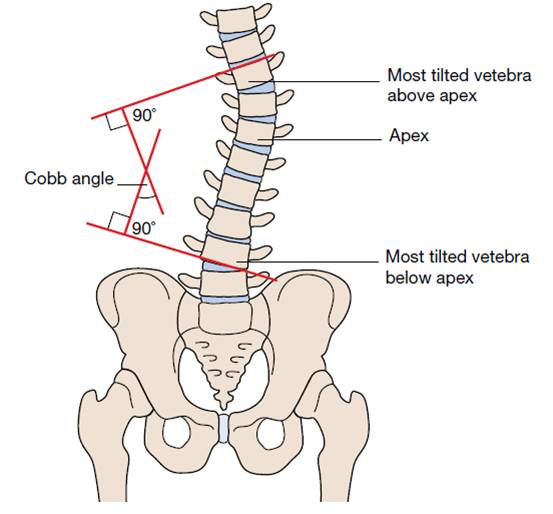
- Measurement of
- Two lines are drawn perpendicular between uppermost and lowest vertebrae involved in the primary curvature
- The angle between the intersecting lines is Cobb’s angle
- Interpretation of Cobb’s angle
- <10o = non-scoliosis
- 10-30o = mild
- 30-45o = moderate
- >45o = severe
MRI
- To rule out intraspinal anomalies
- Indications
- Atypical curve pattern
- Rapid progression
- Neurologic symptoms
- Foot deformities
- Asymmetric abdominal reflexes
Treatment
- Based on the Cobb angle
- Observation – <25o
- Bracing – 25-45o
- Aims to stop progression, rather than correct deformity
- Recommended for between 16-23 hours a day until skeletal maturity
- Obesity and non-compliance reduce outcomes
- Surgery – >45o
- Posterior spinal fusion – gold standard for thoracic and double major curves
- Anterior spinal fusion – for thoracolumbar and lumbar curves
- Anterior and posterior spinal fusion – for Cobb’s angle >75o
Complications
- Neurologic injury
- Infection
- Flat back syndrome
- Superior Mesenteric Artery syndrome