
1. TENOSYNOVITIS
- Inflammation of a tendon and its enveloping sheath (synovium)
Pyogenic/Infective Tenosynovitis
- Infection of the synovial lining of the tendon by bacteria
Epidemiology/etiology
- Most commonly affects the flexor tendon of the fingers
- Bacteria
- S.aureus – most common
- Pasteurella multocida – animal bites
- Eikenella – human bites
- Risk factors – diabetes, IVDU, immunocompromised patients
Pathophysiology
- Mechanisms
- Penetrating trauma to the tendon sheath
- Direct spread from septic joint or deep space infection
- Infection travels in the synovial sheath that surrounds the flexor tendon
Clinical features
- Pain and swelling – localised to palmar aspect of affected digit
- Warmth and redness of affected digit
- Kanavel’s cardinal signs
- Flexed posturing of the involved digit
- Tenderness to palpation over the tendon sheath
- Pain with passive extension of the digit
- Fusiform enlargement of the affected digit
Diagnosis
- Diagnosis is mostly clinical
- Aspiration of joint fluid – for microbial culture
- X-ray – generally not needed, but can be used to rule out other diagnoses
Treatment
- Early presentation – IV antibiotics, analgesia, immobilisation of hand, observation
- Late presentation – incision and drainage, IV antibiotics, analgesia
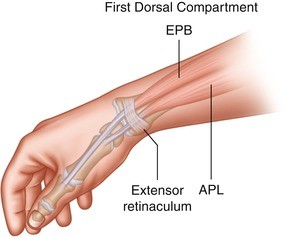
De Quervain’s Tenosynovitis
- A stenosing tenosynovial inflammation of the
- Includes tendons that control the movement of the abductor pollicis longus (APL) and extensor pollicis brevis (EPB)
- Normal functions
- APL – brings thumb forward away from the palm
- EPB – brings the thumb outwards radially
Epidemiology/etiology
- More common in women 30-50 years old
- Most commonly affects the dominant wrist
- Risk factors
- Repetitive movements of the wrist – manual labour, typing, sports
- Post-traumatic
- Post partum
- Rheumatoid arthritis
Pathophysiology
- The APL and EPB tendons are tightly secured against the radial styloid by the overlying extensor retinaculum which creates a fibro-osseous tunnel
- There is non-inflammatory thickening of the retinaculum and tendons from acute or repetitive trauma
- Restrains normal gliding within the sheath
Clinical features
- Gradual onset
- Wrist pain on the radial aspect – exacerbated by gripping objects
- Swelling over the radial aspect of wrist
Diagnosis
- Finkelstein manoeuvre – examiner pulls the thumb of the patient in ulnar deviation and longitudinal traction
- Increased pain in the radial styloid process indicates a positive test
- Eichhoff manoeuvre – pain over radial styloid process when the wrist is ulnarly deviated while patient clenches thumb in fist indicates positive test
- X-ray – generally not needed; can be used to rule out arthritis
Treatment
- Rest, NSAIDs
- Thumb spica splint
- Steroid injections
- Surgical release of 1st dorsal compartment – for patients with severe symptoms
2. TENDONITIS
- Inflammation of a tendon
Epidemiology
- Most common in athletes
- Most common types
- Shoulder – rotator cuff tendonitis, calcific tendonitis, biceps tendonitis
- Elbow – tennis elbow, golfer’s elbow
- Knee – jumper’s knee (patellar tendonitis)
- Ankle – Achilles tendonitis
Etiology
- Repetitive activities – manual labourers, musicians, athletes
- Risk factors – infection, arthritis, gout, diabetes
- Fluoroquinolone antibiotics
Pathophysiology
- Progressive interference of the healing response
- Involves cellular apoptosis, matrix disorganisation and neovascularisation
- Degenerative changes in the collagenous matrix
Clinical features
- Pain over area – exacerbated by motion
- Reduced range of motion
- Swelling
Diagnosis
- Ultrasound
- X-ray
- MRI
Treatment (mostly conservative)
- NSAIDS, rest
- Steroid injections
- Ice, compression, elevation
Physiotherapy