
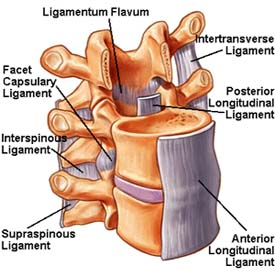
- AKA Potts disease
- Characterised by vertebral body osteomyelitis and intervertebral discitis as a result of tuberculosis
Epidemiology
- Most common in Asia and sub-Saharan Africa
- Spine is the most common location of musculoskeletal TB – especially thoracic spine
- Associated co-morbidities – HIV/AIDS, immunosuppression, peptic ulcer, alcoholism, malnutrition
Etiology
- Causative organism – Mycobacterium tuberculosis
- Due to haematogenous spread of pulmonary TB
- Can also spread through lymphatics
- Once spread, the infection can target vertebrae, intervertebral discs, epidural or intradural space
Pathogenesis
Early infection
- Spreads under the and leads to
- Contiguous multilevel involvement
- Skip lesion or noncontiguous segments
- Paraspinal abscess formation
- Early infection does not involve the disc space
Chronic infection – leads to severe kyphosis
- In adults – kyphosis remains static after healing of the disease
- In children – kyphosis can progress due to growth spurts
Types –
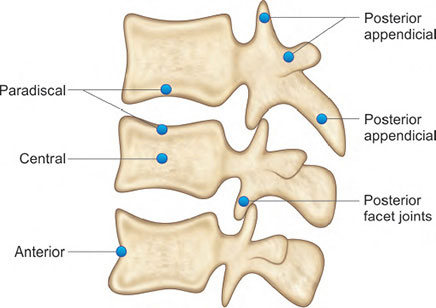
Paradiscal – most common
- Primary focus of infection is the vertebral metaphysis
- erodes the cartilaginous endplate and narrows the disc space
Anterior granuloma – granuloma develops underneath the anterior longitudinal space
- Less bone destruction but more bone devascularisation
- Further development of abscess, necrosis and deformity
Central lesions – involves entire vertebral body, affecting >2 vertebrae
- Causes significant deformities and pathologic fractures
Appendiceal type lesions – affects lamina, pedicles, articular facets and spinous processes
Clinical features
- Symptoms are more insidious compared to a pyogenic infection
- Constitutional symptoms – malaise, night sweats, night sweats, low grade fever
- Back pain – often a late symptom
- Kyphosis
- Neurologic deficits – due to mechanical pressure on spinal cord by abscess, granulation and caseous tissue
- Paraplegia, paresis, impaired sensation, nerve root pain, cauda equine syndrome
- More common in patients with cervical spine TB
Diagnosis
- Mantoux test (Tuberculin skin test) – injection of a purified protein derivative (PPD)
- Positive in 90% of cases
- Microbiology – bone tissue/abscess samples obtained
- Stained for acid-fast bacilli
- X-ray
- Lytic destruction of anterior part of vertebral body
- Collapse of vertebral body
- Disc space destruction
- Shadows suggestive of abscess formation
- CT – better at defining lesions <1.5cm
- MRI – gold standard for diagnosis
- Shows smooth walled abscess
- End-plate disruption
- Spinal cord edema and atrophy
Treatment
Pharamacologic
- Indications – in absence of neurologic deficits
- Drugs – Isoniazid (H), Rifampin (R), Ethambutol (E), Pyrazinamide (Z)
- Regimen – HRZE for 2 months, followed by HR for 9-18 months
Operative – indicated if there is spinal instability, neurological deficits or cord compression
- Indications – spinal instability, neurological deficits, cord compression, severe kyphosis
- Anterior decompression/corpectomy – done in 2 stages
- Anterior decompression with bone grafting
- Posterior kyphosis correction and instrumentation
- Halo traction, anterior decompression, bone grafting, anterior plating – for cervical kyphosis
- Pedicle subtraction osteotomy – for lumbar kyphosis
Complications
- Deformity
- Retropharyngeal abscess
- Respiratory compromise
- Pott’s paraplegia – spinal cord injury due to abscess
Differential diagnosis
- Pyogenic infection – causes more destruction of intervertebral disc space, forms larger abscesses and has systemic involvement of multiple organs
- Brucellosis
- Funal infection
- Sarcoidosis
- Metastasis