
- Breach in the integrity of the aortic wall
- Allows arterial blood to enter the media, which is then split into two layers – creates a ‘false lumen’
- The false lumen eventually re-enters the true lumen – creates a double-barrelled aorta
- But it can also rupture into the left pleural space or the pericardium – fatal
Etiology
- Hypertension – MC
- Aortic atherosclerosis
- Aortic coarctation
- Connective tissue disorders – Marfan’s
- Previous aortic surgery – CABG, valve replacement
- Iatrogenic – cardiac catheterisation, IABP
Clinical features
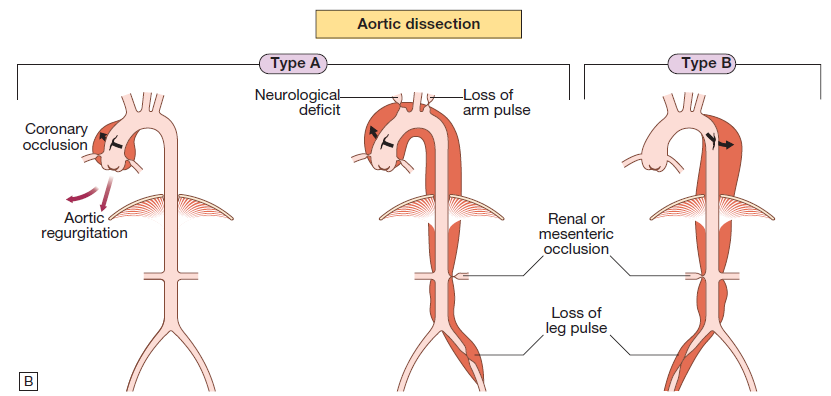
- Involvement of ascending aorta – chest pain
- Descending aorta – intrascapular pain
- Pain – tearing, abrupt onset
- Pt is hypertensive unless there is major haemorrhage
- Asymmetry of the brachial, carotid, femoral pulses
- Occlusion of aortic branches can cause – MI (coronary), stroke (carotid), paraplegia (spinal), mesenteric infarction with acute abdomen (celiac and sup mesenteric), renal failure (renal)
Diagnosis
- CXR – widening of mediastinum, distortion of aortic knuckle, pleural effusion
- ECG – LVH in pts with HTN
- Doppler Echo – aortic regurgitation, dilated aortic root
- TOE
Management
- Pain control and anti-hypertensive tx
- Type A – emergency surgery to replace ascending aorta
- Type B – treated medically unless there is impending rupture or organ ischemia
- Aim of medical management is to maintain MAP of 70mmHg to reduce force of ejection of blood from LV
- BB + α-blockers
- CCB – verapamil, diltiazem
- Endoluminal repair – involves fenestrating the intimal flap so blood can return from the false lumen to the true