
Etiology
- Infants, children, adolescent
- Young adults to middle-aged
- Calcification and fibrosis of a congenitally bicuspid valve
- Rheumatic aortic Stenosis
- Elderly
- Senile Calcification (MCC of AS)
- Rheumatic AS
Pathogenesis
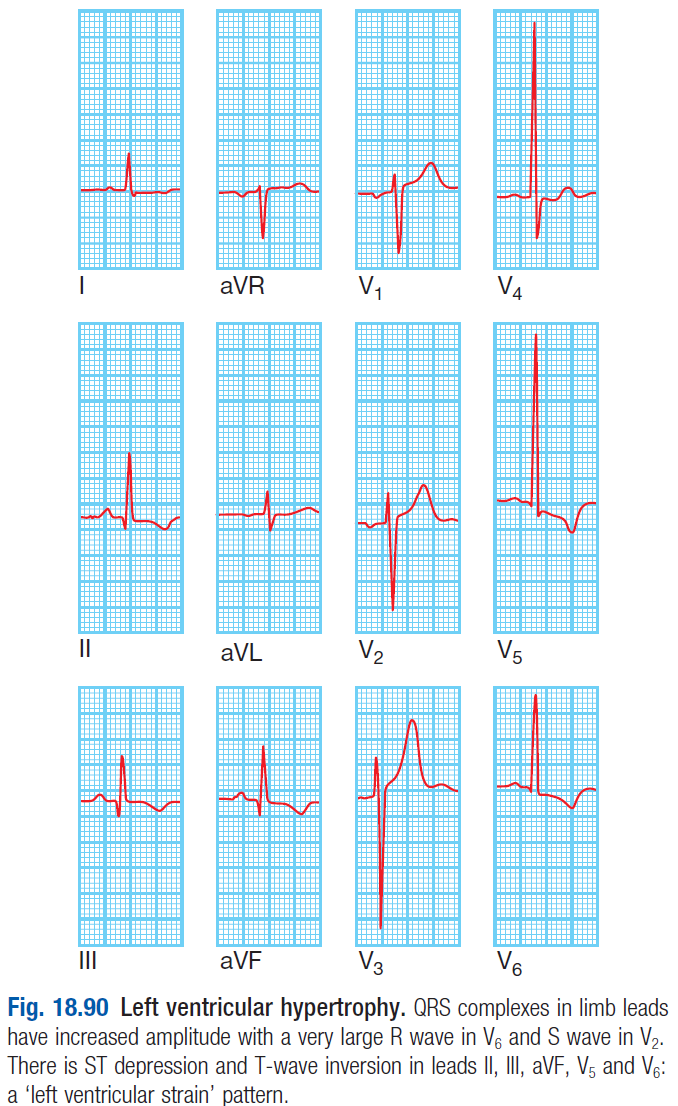
- Obstructed LV emptying leads to ↑LVP – causing LVH (ECG changes show Tall R waves, SV1 +RV5 = >35mm)
- Results in ischemia of the LV myocardium – causing angina, arrhythmias and LV failure
- Obstruction to LV outflow becomes more severe on exercise
- In AS, cardiac output hardly increases during exercise
- Results in ↓BP and coronary ischemia worsens
- Eventually, LV can no longer overcome outflow tract obstruction
- Results in pulmonary oedema
- In contrast to pts with MVS, pts with AS remain asymptomatic or years but deteriorate rapidly when sx develop
- Death within 3-5 years of symptoms
Clinical features
- 3 cardinal symptoms – angina, breathlessness, syncope
- Harsh ejection systolic murmur
- Slow rising carotid pulse
- Thrusting apex beat – due to LV pressure overload
Diagnosis
ECG – ‘LLL’
- LV hypertrophy
- LV strain – ST dep and T wave inversion in II, III, aVF, V5, V6
- ↑QRS amplitude and tall R waves
- LBBB
- Left axis deviation
Echo (diagnostic) – shows restricted valve opening
Doppler – shows the pressure gradient across the valve
Cardiac catheterisation
- To identify associated coronary artery disease
Treatment
- Keep asymptomatic patients under review for development of angina, syncope and dyspnoea
- Aortic valve replacement – for pts with symptomatic severe AS
- Anticoagulants – for patients who have AF
- Balloon dilation
- Prophylactic antibiotics for infective endocarditis